Hepatitis A and E
Hepatitis A and Hepatitis E
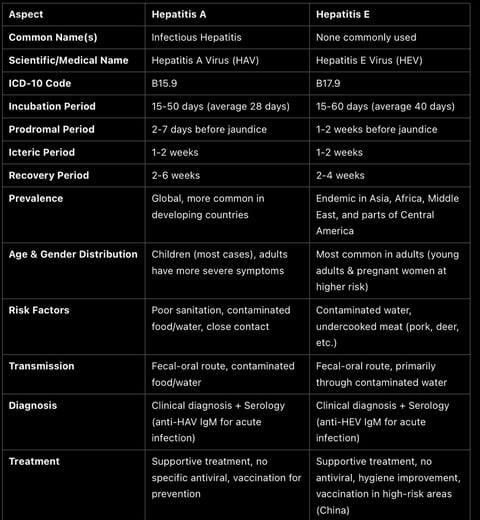
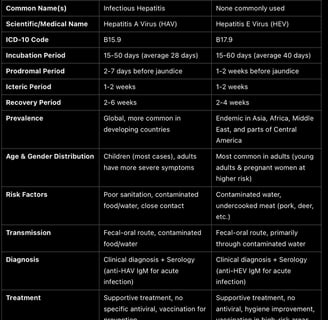
1. Overview
• Hepatitis A and Hepatitis E are both viral infections that primarily affect the liver. They share similar modes of transmission, clinical manifestations, and self-limiting nature in most cases. However, they are caused by distinct viruses and have some differences in their epidemiology, clinical course, and complications.
2. Etiology
• Hepatitis A:
• Caused by: Hepatitis A virus (HAV), a single-stranded RNA virus from the Picornaviridae family.
• Transmission: Fecal-oral route, typically via contaminated food or water or direct person-to-person contact.
• Hepatitis E:
• Caused by: Hepatitis E virus (HEV), a single-stranded RNA virus from the Hepeviridae family.
• Transmission: Fecal-oral route, similar to Hepatitis A, often due to contaminated water sources, especially in areas with poor sanitation.
3. Epidemiology
• Hepatitis A:
• Global Prevalence: More common in regions with poor sanitation, such as parts of Asia, Africa, and Latin America. Its incidence has declined significantly in developed countries due to vaccination and improved sanitation.
• At-Risk Groups: Travelers to endemic areas, MSM, individuals in close contact with infected individuals, children in developing regions.
• Hepatitis E:
• Global Prevalence: Endemic in many developing countries, particularly in South and East Asia, Sub-Saharan Africa, and the Middle East. HEV outbreaks are common during the rainy season.
• At-Risk Groups: People living in areas with inadequate sanitation and contaminated water, pregnant women (particularly in the third trimester), and immunocompromised individuals.
4. Clinical Features
• Hepatitis A:
• Symptoms:
• Jaundice (yellowing of skin/eyes)
• Fever
• Fatigue
• Abdominal discomfort (especially in the right upper quadrant)
• Dark urine and pale stools
• Nausea and vomiting
• Progression: Generally mild with most patients recovering within 2-6 months without chronic liver damage.
• Hepatitis E:
• Symptoms:
• Jaundice
• Fever
• Abdominal pain
• Nausea and vomiting
• Dark urine and pale stools
• Pruritus (itchy skin)
• Progression: While most cases are self-limiting, it can be severe in pregnant women, particularly in the third trimester, leading to high mortality rates.
5. Pathophysiology
• Hepatitis A:
• The virus enters the body through the gastrointestinal tract, travels to the liver via the bloodstream, and infects hepatocytes. The liver’s immune response leads to inflammation and damage to the liver cells, causing the classic symptoms.
• Hepatitis E:
• Similarly, HEV is ingested through contaminated water or food, travels to the liver, and replicates in hepatocytes. The immune response causes inflammation. In most individuals, the infection is self-limiting, but in pregnant women and immunocompromised individuals, it can cause acute liver failure.
6. Diagnosis
• Hepatitis A:
• Serology: Elevated levels of ALT, AST, bilirubin.
• HAV IgM antibodies in the blood indicate acute infection.
• HAV RNA PCR is used in some cases for confirmation.
• Hepatitis E:
• Serology: Elevated liver enzymes (ALT, AST), bilirubin.
• HEV IgM antibodies and HEV RNA PCR are used to confirm active infection.
• Liver biopsy in severe cases may show signs of acute hepatitis.
7. Differential Diagnosis
• Both Hepatitis A and Hepatitis E must be differentiated from other causes of hepatitis, such as:
• Hepatitis B and C
• Alcoholic hepatitis
• Autoimmune hepatitis
• Non-alcoholic fatty liver disease (NAFLD)
8. Complications
• Hepatitis A:
• Acute liver failure is rare but possible, especially in older adults or those with pre-existing liver disease.
• Chronic liver disease does not occur.
• Hepatitis E:
• Acute liver failure may occur, particularly in pregnant women, and can be fatal (especially in the third trimester).
• Chronic infection is extremely rare, but it can occur in immunocompromised individuals.
9. Treatment
• Hepatitis A:
• No specific antiviral treatment is available.
• Supportive care (hydration, pain management, rest) is the mainstay of treatment.
• Liver function tests and monitoring for complications (like coagulopathy or encephalopathy) are important.
• Hepatitis E:
• Like Hepatitis A, there is no specific antiviral treatment for Hepatitis E.
• Supportive care is provided, especially for those with severe disease.
• In pregnancy, delivery of the fetus may be considered in cases of severe disease, depending on gestational age.
10. Prevention
• Hepatitis A:
• Vaccination is highly effective and recommended for travelers to endemic areas, individuals with chronic liver diseases, and MSM.
• Improved sanitation and hygiene (handwashing, safe food and water practices) are critical in preventing transmission.
• Hepatitis E:
• No vaccine is available in most countries, though there is a licensed vaccine in China.
• Improved sanitation and clean drinking water are essential for prevention.
• Avoiding consumption of undercooked or raw meat from infected animals (especially pork) can help reduce risk.
11. Prognosis
• Hepatitis A:
• The prognosis is generally excellent with most patients recovering fully within 2-6 months.
• The risk of chronic liver disease is virtually nonexistent.
• Hepatitis E:
• Mild cases resolve within a few weeks, with the majority of people making a full recovery.
• Severe cases, particularly in pregnant women, can result in liver failure and death.
12. Public Health Considerations
• Hepatitis A:
Hepatitis A vaccination programs have helped reduce the incidence in many developed countries. Improved sanitation and clean water access are key to controlling outbreaks in endemic regions.
• Hepatitis E:
Hepatitis E outbreaks are often linked to poor water quality, especially during the rainy season. Efforts to improve water and sanitation infrastructure in endemic regions are crucial.
Hepatitis A & Hepatitis E: Key Periods (Concise)
Hepatitis A
1. Incubation Period:
• 15-50 days (average: 28 days)
2. Prodromal Period (Initial Phase):
• 2-7 days before jaundice
• Symptoms: Fatigue, anorexia, nausea, vomiting, fever, right upper quadrant pain.
3. Icteric Period (Jaundice Phase):
• 1-2 weeks
• Symptoms: Jaundice, dark urine, pale stools, elevated liver enzymes.
4. Recovery Period:
• 2-6 weeks
• Most recover completely without chronic complications.
Hepatitis E
1. Incubation Period:
• 15-60 days (average: 40 days)
2. Prodromal Period (Initial Phase):
• 1-2 weeks before jaundice
• Symptoms: Fatigue, anorexia, fever, abdominal pain, nausea.
3. Icteric Period (Jaundice Phase):
• 1-2 weeks
• Symptoms: Jaundice, dark urine, pale stools, elevated liver enzymes.
4. Recovery Period:
• 2-4 weeks
• Most cases resolve without chronic disease, but severe cases can lead to liver failure (especially in pregnant women).